Hormone Testing for Lactation
There are many reasons to do hormone testing for breastfeeding. These may be past or present supply issues or because of concern due to hormonal imbalance issues -such as PCOS, past blood sugar issues, thyroid concerns, fertility challenges, etc. It is important that these tests be thorough so that a whole picture assessment can be made. It is also important that the results be examined through the lens of normal levels during lactation, which are different from any other time. While the testing can be ordered by anyone able and willing, any action taken to resolve abnormal results, should involve someone who is an expert in the hormones of lactation, like an IBCLC.
In addition to the labs below, a CBC, CMP, and ferritin can be very helpful.
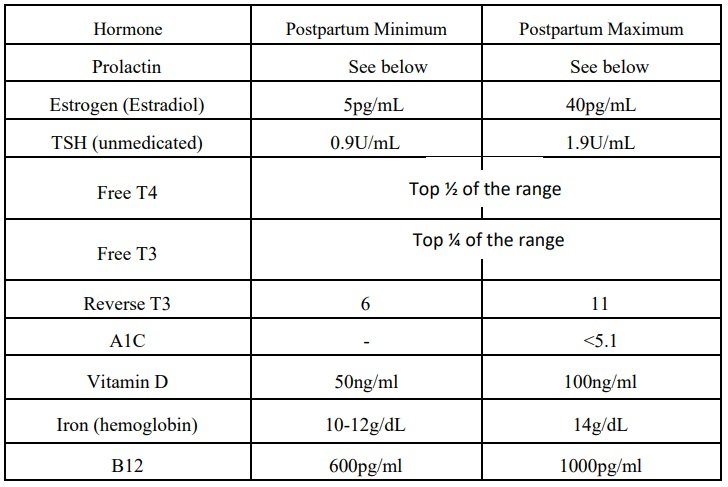
Testing Prolactin levels is a little more complicated than most things. Ideally 2 levels are checked; baseline and responsive. Baseline is taken (via blood draw) at least 2 hours post nursing/pumping. Responsive is taken 45 minutes from starting a nursing/pumping session immediately following the baseline draw. Here are the minimums for baseline at different points postpartum. Responsive should roughly be double baseline or higher. Other things it might be helpful to add would be HCG, Testosterone, Growth Hormone, and Iodine. Prenatally, 2 weeks, 6 weeks and 12 weeks postpartum are important times for a person with risk factors, like a history of Gestational (or other) diabetes, PCOS, or thyroid issues.

When considering when to test it is helpful to know that there are major hormone shifts 9 days after birth, 6 weeks, 3 months, and 14 months. Changes can also occur due to external factors such as medication, galactagogues, health issues (especially gut health), reduction/increase in nursing, effectiveness of baby at the breast, degree of solids being eaten, onset of fertility postpartum, pregnancy, or even, occasionally, diet. Ultimately, just one of these numbers only gives you one piece of the puzzle. Having less than a full panel run compromises care. If one level is off or a lot are borderline, all values need to be considered. Beyond this, symptoms are wise to include as well. Every individual is unique and should be looked at as such. Find the right person to support you in working through any possible hormone issues, as the treatment options are going to be numerous too. With good information and support, understanding the hormones supporting lactation need not be overwhelming!
All of this is a quick, superficial overview of labs and ranges. Professionals who would like to understand these in far more depth are encouraged to start with The Thyroid and Lactation class offered periodically throughout the year. While diving most deeply into thyroid function, this course includes information on several of these other things, as well as details on how to make sure that lab results are accurate and tools for addressing labs that might be found to be negatively affecting milk supply.
Parents who are interested in understanding their own labs, and next steps to take, can also get help from Bliss At The Breast.
A few of many References:
Cox, D., Owens, R., Hartmann, P. Blood and milk prolactin and the rate of milk synthesis in women. 1996 DeCarvalho, M., Robertson, S., Friedman, A., et al. Effect of frequent breast-feeding on early milk production and infant weight gain. Pediatrics 1983
Gottfried, Sara. The Hormone Cure. New York, NY: Scribner, 2013 Lawrence, R. Breastfeeding: A Guide for the Medical Profession . 6th ed. Philadelphia, PA: Elsevier Mosby Noel GL, Suh HK, Frantz AG.
Prolactin release during nursing and breast stimulation in postpartum and non-postpartum subjects. J Clin Endocrinol Metab. 1974 Mar;38(3):413-23.
West, D., Marasco, L. The Breastfeeding Mother’s Guide to Making More Milk , New York: McGraw-Hill, 2020
Hennessey JV, Espaillat R. Current evidence for the treatment of hypothyroidism with levothyroxine/levotriiodothyronine combination therapy versus levothyroxine monotherapy. Int J Clin Pract. 2018;72(2):e13062. doi:10.1111/ijcp.13062
Panuganti PL, Hinkle SN, Rawal S, et al. Lactation Duration and Long-Term Thyroid Function: A Study among Women with Gestational Diabetes. Nutrients. 2018;10(7):938. Published 2018 Jul 21. doi:10.3390/nu10070938

www.StopTheThyroidMadness.com
https://chriskresser.com/how-to-prevent-diabetes-and-heart-disease-for-16/